Home Hospice Care
The Saint Luke’s Hospice team helps make patients’ final days a time of comfort and love. We walk with patients and families throughout the journey—helping manage the physical, emotional, and spiritual care needed at end of life, allowing them to focus on spending quality time together.
We provide individualized care in patients' homes or in an assisted living or nursing facility. Our team of hospice experts uses the latest clinical best practices and holistic approaches—such as music, pet, or aroma therapy—to manage patients’ pain and other symptoms, making them as comfortable as possible.
Our team also supports patients’ loved ones while they come to terms with their loss. Grief coordinators, chaplains, and other experts are with them through the stages of grief. They help prepare the family for the process of dying and can provide support one-on-one, or through our Café Hope grief support group.
Hospice patients and their families have all-day and all-night access to their care team.
For patients that need more intensive care, we offer Saint Luke’s Hospice House.
Our hospice team is experienced, trained, and passionate about the quality of every day of each patient’s life.
Call 816-756-1160 for more information.
Hospice Services
- Pain and symptom management
- Dietary and nutrition services
- Specialized programs such as music and pet therapy
- Educational resources for families on death and dying
- Qualifying medical equipment, supplies, and medication may be included
- Ongoing grief support for family members before and after a loved one’s passing
Who Can Benefit from Hospice
Our dedicated admissions team has expertise in communicating with patients and families about hospice care. Hospice services require an evaluation and physician’s order for admission.
Our rapid-response, same-day admission process offers convenience and reassurance to those who need immediate help.
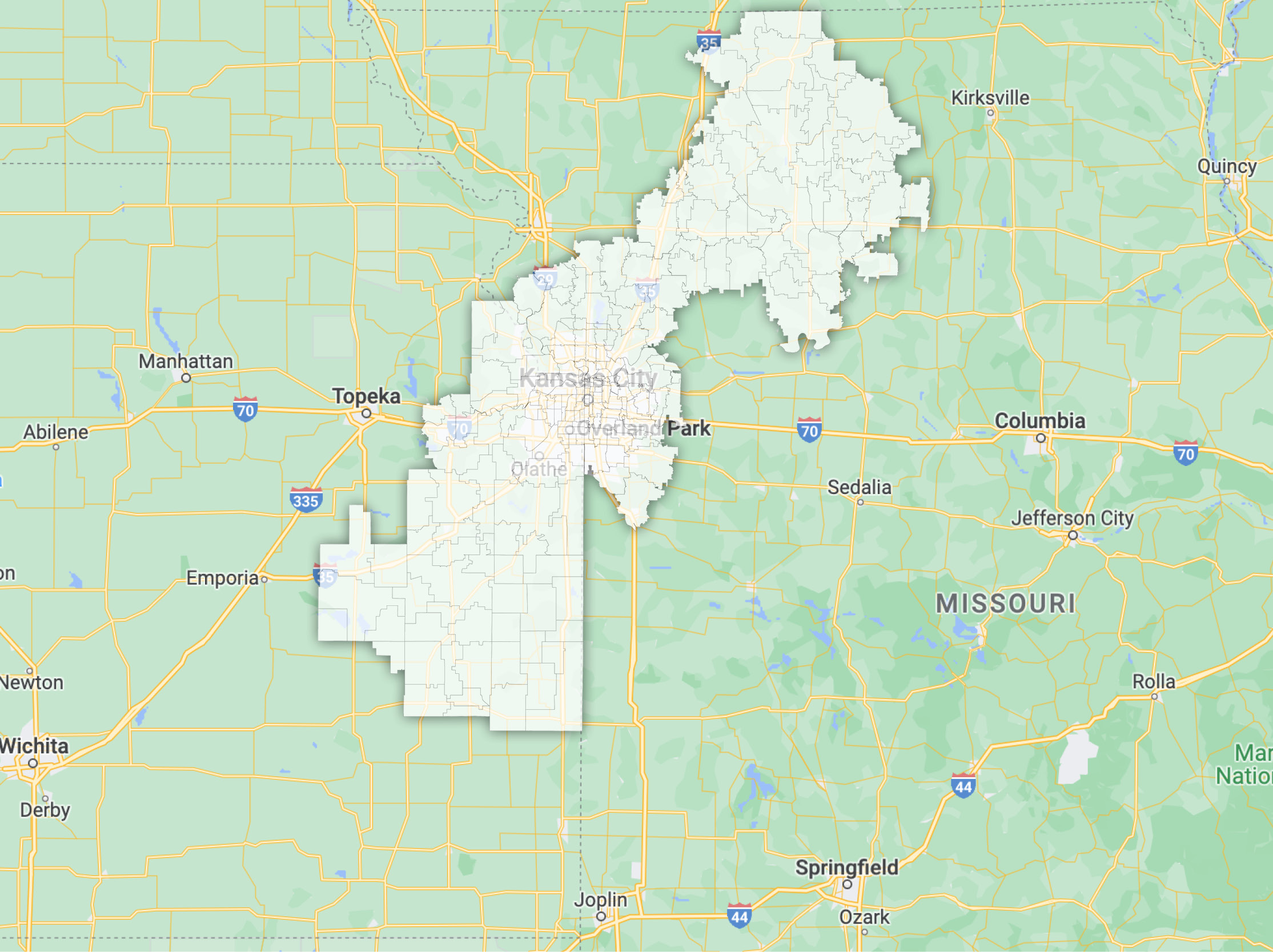
Service Area
Licensed Counties in Kansas
- Allen
- Anderson
- Bourbon
- Coffey
- Douglas
- Franklin
- Johnson
- Leavenworth
- Linn
- Miami
- Wyandotte
Licensed Counties in Missouri
- Caldwell
- Carroll
- Cass
- Chariton
- Clay
- Clinton
- Daviess
- Grundy
- Harrison
- Jackson
- Johnson
- Lafayette
- Linn
- Livingston
- Mercer
- Platte
- Ray
- Sullivan
Relevant News
News
FOX 4: The Afternoon Drive: Handling Grief During the Holidays
News
Home Care & Hospice South Branch Office Moves to Anderson County
Article
Do Your Loved Ones Know Your Wishes?
Article